
APDW 2015:The diagnosis and treatment of early colorectal cancer and precancerous lesions
In December 2015 on the 3rd meeting of the Asia Pacific Digestive Disease Week (apdw) on both sides of the Taiwan Straits digestive endoscopy forum, cross-strait endoscopic experts gathered, digestive tract diseases of endoscopic diagnosis and treatment in-depth exchanges and explore, will, Professor Jiang Bo, Beijing Tsinghua Chang Gung Memorial Hospital digestion head of the medical department is early colorectal cancer and precancerous lesions of endoscopic diagnosis and therapy related issues delivered a speech.
Professor Jiang described the epidemiology, diagnostic methods, endoscopic monitoring and treatment of colorectal cancer. Professor Jiang believes that with the continuous improvement of people's living standard in our country and eating habits change, the incidence of colorectal cancer in China rate also increased year by year, so early colorectal cancer and precancerous lesions of endoscopic diagnosis and treatment in the diagnosis and treatment of gastrointestinal tumor also plays a more and more important role.
Diagnosis, Professor Jiang mentioned the magnifying colonoscopy technology combined with the gland orifice type (pit pattern, figure 1), determine the nature of the lesions, made the same height and pathological diagnosis.
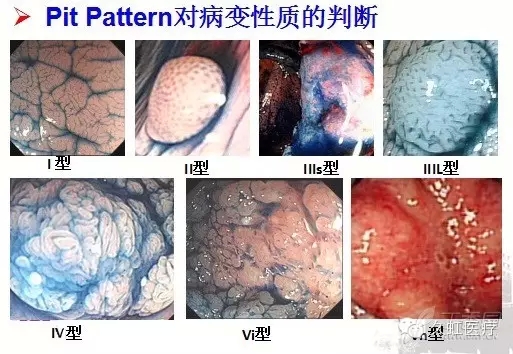
Figure 1. Pit Pattern Judgment on the nature of the lesion
Staining magnifying endoscopy combined with crystal violet staining (Figure 2) can effectively determine the depth of invasion and the nature of the lesion, so as to determine the endoscopic treatment plan. Professor Jiang stressed that attention should be paid to the diagnosis of flat lesions.
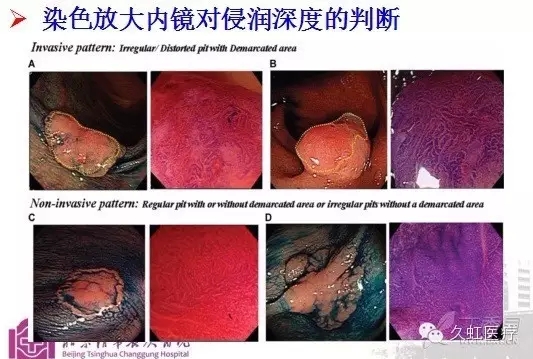
Figure 2. The judgment of the depth of infiltration by staining magnifying endoscopy
Professor Jiang also referred to the endoscopic diagnosis of colorectal cancer, and for the related diseases and cancer of the missed diagnosis problems put forward a clear response measures:
1 for the first time, it should be followed up in one year after the discovery of large polyps;
The 2 line has larger polyps resection should be in 3 to 6 months to clear the completeness of resection of colonoscopy;
3 follow-up doctor qualification should be improved, the condition is high year endowment doctor, should pay attention to the occurrence of flat tumor, strengthen the application of dyeing endoscope;
. population of colorectal polyps with high-risk groups, it is recommended follow-up time: polyp is found, a year review; still, a year to review; no interval of 3 years; no, interval of 5 years; no, interval of 10 years; follow-up note interval cancer occurrence.
In the surveillance of colorectal cancer, Professor Jiang said, ulcerative colitis is a risk factor for colorectal cancer, it should pay special attention to this part of the patient's screening. And should pay attention to the early stage of colorectal cancer and precancerous lesions, and pay attention to the pit typing of the tumor.
Regarding the treatment of early colorectal cancer and precancerous lesions, Professor Jiang believes that the ESD of colorectal tumors en bloc resection rate and total resection rate is far higher than EMR. Finally, Professor Jiang made a summary of the wonderful content of the lecture, it is recommended to work hard in order to achieve a precise treatment of early colorectal cancer and precancerous lesions.
Finally, Professor Jiang summed up the main points of the endoscopic treatment of colorectal cancer and precancerous lesions:
The picture is provided with Professor Jiang.
 TOP
TOP